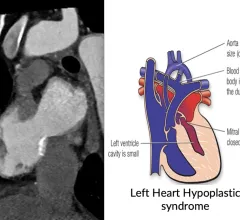
Carotid artery disease causes up to 30% of all strokes, but severely calcified lesions can make treatment quite complex. The hope is that IVL can be as successful in this area as it has been in the treatment of coronary and peripheral artery disease.
Matthew Reynolds, MD, Lahey Hospital and Medical Center, explains data from the EXCALIBER and CAMELOT studies that show ambulatory cardiac monitoring usage among more than 300,000 patients.
Gene manipulation can revert the cardiomyocytes back to a fetal state, allowing them to regenerate. Researchers are now looking for drugs to mimic the effect.
The publication will include "pictorial essays, case reports and expert commentary for today’s practicing radiologists," the society announced Thursday.
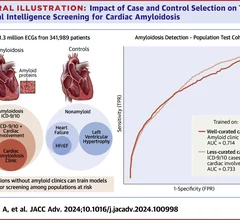
Early detection of cardiac amyloidosis is leads to the best outcomes, but it is often missed until later stages. AI is being developed to help detect these patients earlier using ECG and echo.
Researchers explored data from 23 different studies, identifying a “positive and almost linear association” between alcohol consumption and hypertension.
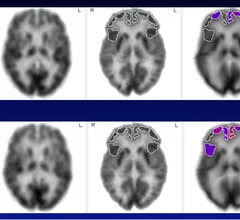
A new study suggests sildenafil, known by its brand name Viagra, can improve cerebrovascular function and minimize the risk of cognitive impairment caused by small vessel disease.
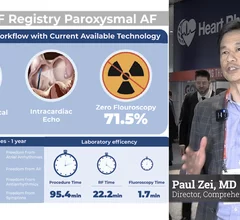
Paul Zei, MD, discusses late-breaking data from the REAL-AF Registry, which looked at the short- and long-term outcomes of radiofrequency ablation in paroxysmal and persistent atrial fibrillation.



![Performing transcatheter aortic valve replacement (TAVR) with the J-Valve transcatheter heart valve (THV) may help limit the risk of coronary artery obstruction (CAO) in high-risk patients, according to a new study published in Clinical Interventions in Aging.[1]](/sites/default/files/styles/top_stories/public/2024-10/screenshot_2024-10-01_at_2.16.21_pm.png.webp?itok=kSiGReBW)